Posted June 16, 2025 in Fertility Blog & Information
14 minute read
Key Takeaways
- Asherman’s Syndrome develops when scar tissue, or adhesions, grow within the uterus. It usually occurs after surgery or infection and may disrupt menstrual cycles and fertility.
- Timely diagnosis via fertility evaluation, imaging, and hysteroscopy are crucial in diagnosing and staging the severity of adhesions.
- The treatment of Asherman’s syndrome primarily consists of minimally invasive hysteroscopic surgery to excise scar tissue, then subsequent medical management and long-term surveillance.
- Hormonal therapy plays a crucial role in recovery. Supportive healing therapies — such as physical therapy or acupuncture — are useful in preventing recurrence.
- Lifestyle changes to improve uterine health and fertility post treatment! Keep your weight down, have a nutritious diet, stay physically active and don’t smoke.
- Support from specialists, mental health professionals, and patient advocates is integral. They are crucial partners in your care, helping with the physical and emotional journey of AS.
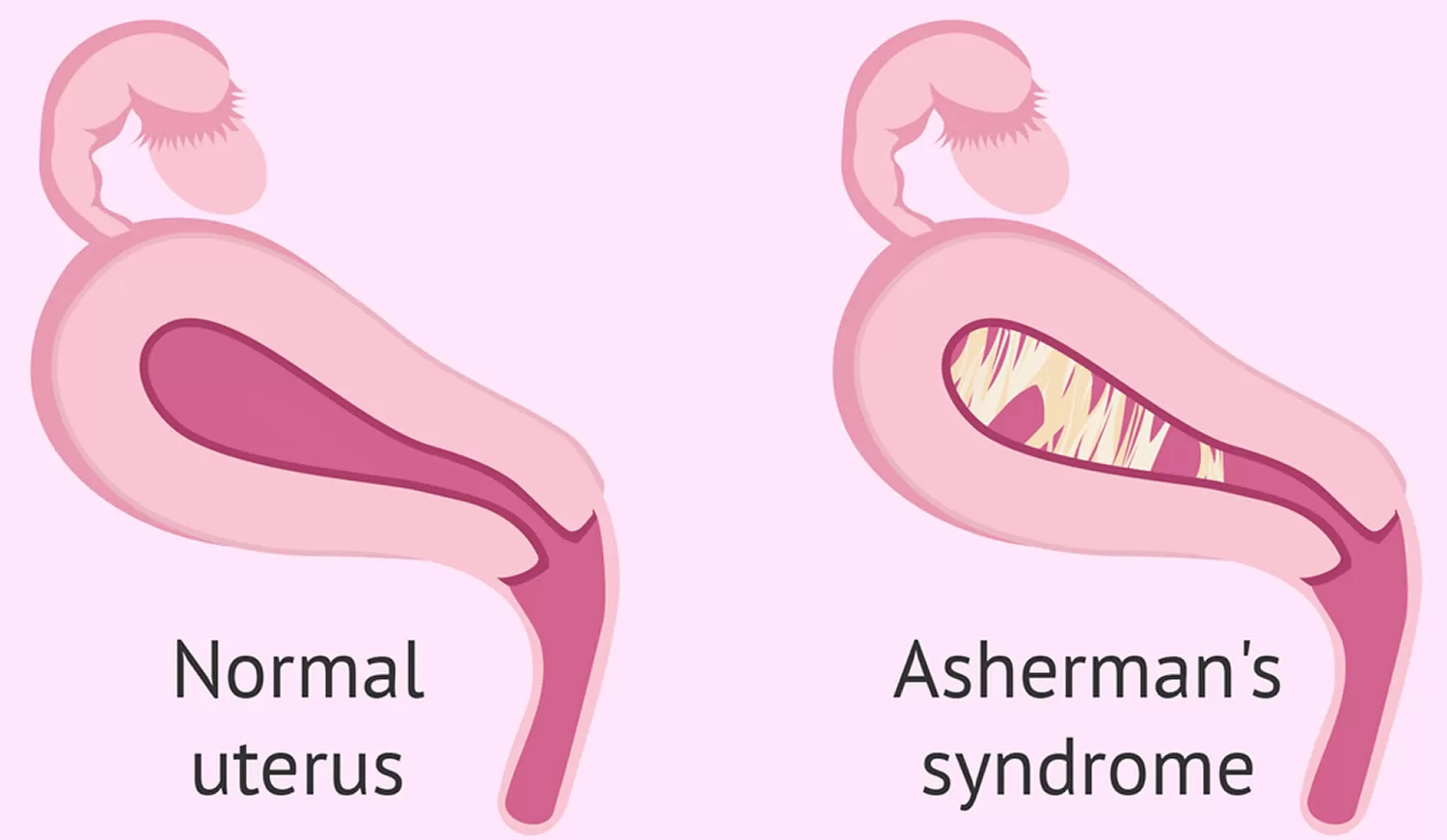
Asherman’s syndrome is an often misdiagnosed chronic health condition characterized by the development of adhesions, or scar tissue, within the uterus. This very painful condition usually results in painful menses and difficulty achieving and/or maintaining pregnancy.
In the United States, doctors usually test for Asherman’s syndrome through a pelvic exam or an ultrasound. They can do a specific test, hysteroscopy, that lets them look inside the uterus.
Treatment usually includes surgically removing the scar tissue. After having the tissue removed, the majority of women will require ongoing care to stop the tissue from returning.
Early identification and effective treatment is crucial to restoring fertility potential. Women want to know straightforward, simple answers about what these steps are going to mean.
This guide covers how physicians diagnose and treat Asherman’s syndrome to restore fertility.
What Is Asherman’s Syndrome?
Asherman’s Syndrome, called intrauterine adhesions, is a rare disease characterized by the presence of scar tissue—called adhesions—throughout the uterus. These adhesions can lead to the walls of the uterus sticking to one another. This usually alters regular menstrual periods and may even lead to infertility.
The condition typically starts following an injury to the uterus. Usually, this happens after surgical procedures such as dilation and curettage (D&C). Dr. Joseph Asherman was the first to describe this syndrome in the mid-20th century. Since then, his name has been inextricably tied to it.
Scar Tissue Inside Uterus
Scar tissue is the body’s natural response when the uterus is injured. This may occur after fibroid-removal surgeries, such as D&C, myomectomy, or a C-section. If left untreated, this tissue can occlude portions of the uterus.
This obstruction creates difficulty for periods to occur or for a pregnancy to implant. Women will find their periods are lighter, or they stop having them altogether. This may happen when the uterus is unable to properly shed its lining, leading to painful periods or even potentially severe complications.
These adhesions can cause recurrent miscarriage, as embryos cannot implant in a healthy endometrium.
How Does It Happen?
The leading culprit is surgical fibroids and polyps removal. This is a result of infections, and even specific parasites, such as blood flukes, can cause this.
In other parts of the world, infectious etiologies like genital tuberculosis are more prominent. Other times, individuals might be predisposed to developing this syndrome due to genetics or autoimmune disorders.
Spotting the Warning Signs
The main warning signs are changes to your period—such as a significantly lighter flow or amenorrhea (absence of menstruation). Persistent pelvic pain may be another tip-off.
Having recurrent miscarriages or difficulty conceiving can indicate Asherman’s Syndrome.
Understanding Your Risk Factors
Your risk increases if you’ve had previous uterine surgery, are of advanced maternal age, and/or have other medical conditions. Smokers and those who are obese are at an increased risk as well.
Rates are higher in areas where infections are endemic.
Diagnosing Asherman’s: Uncovering Answers
Diagnosing Asherman’s Syndrome requires collaboration on the part of any patient and their knowledgeable provider. Clinical evaluation remains the gold standard. Physicians begin with a thorough medical history, inquiring about any previous uterine surgeries, recent miscarriages, or changes to menstrual cycles.
These signs of Asherman’s can indicate the presence of scar tissue inside the uterus. A complete physical examination will help to rule out other potential causes of infertility or menstrual irregularities. Differential diagnosis prevents us from landing on an answer — any answer — instead of the correct one.
1. First Clues: Fertility Tests
- Hormone panels
- Transvaginal ultrasound
- Hysterosalpingogram (HSG)
- Saline infusion sonography (SIS)
- Endometrial biopsy
These tests examine whether the uterus and ovaries are functioning properly. For instance, an HSG can identify whether there’s any blockage in the uterine cavity, whereas an ultrasound will demonstrate the interior shape of the uterus.
These fertility tests identify issues early on to prevent further damage.
2. Seeing Inside: Imaging Options
HSG (hysterosalpingogram) uses a dye and X-ray to outline the uterus. This can reveal openings or obstructions in which the adhesions might lie.
Sonohysterography takes it a step further, injecting saline into the cavity to distend it and provide a better view of the inside. These diagnostics are incredibly useful in determining whether scar tissue is indeed present and, if so, its location.
3. Hysteroscopy: The Gold Standard
Hysteroscopy simply refers to the insertion of a small camera into the uterus. It’s safe, minimally invasive, and significantly reduces healing time while allowing doctors to see and treat adhesions immediately.
This is what makes it the gold standard for diagnosing and removing Asherman’s.
4. Staging Adhesion Severity
Doctors consider how thick and where the scar tissue is located. Staging not only assists in planning treatment, but allows for an educated prediction of future fertility success.
The more scars there are, the harder it is for them to restore fertility.
5. Adhesion Location & Fertility
Where scars form in the uterus matters. Scars near the top can block embryo implantation, while those near the cervix can stop periods.
Treatment plans start with the knowledge of these results.
Treating Asherman’s: Restoring Fertility
Restoring fertility in people with Asherman’s Syndrome usually begins with an outpatient procedure to remove scar tissue from the uterus. Their ideal form of treatment varies based on the extent of scar tissue as well as the individual’s desire to have children.
Though surgery is the cornerstone, preoperative medical management and postoperative care are equally important to achieve the best long-term outcomes.
Surgical Adhesion Removal
Nearly all physicians performing hysteroscopic adhesiolysis remove uterine scar tissue with scissors or laser. In the technique, doctors insert a thin scope and smaller tools.
These tools allow them to visualize and excise the bands obstructing the uterus. This work is very sensitive. It takes a very skilled hand and can risk complications like infection or creating a hole in the uterus.
The recovery time is usually short, with the majority of patients returning to normal within one week. If adhesions return, revision surgery may be required.
Preventing Scar Re-Growth
To prevent re-adhesion of uterine walls, several strategies can be employed.
- Insert a balloon or IUD to prevent re-adhesion of uterine walls.
- Use short-term antibiotics to prevent infection.
- Schedule early follow-up hysteroscopy to check healing.
- Apply estrogen to help the lining regrow.
- Avoid procedures that could cause new injury.
Consistent follow-up care can identify issues before they escalate. Providing proper education on warning signs and steps for recovering significantly reduces the risk of scars re-growing.
Hormones: Aiding Recovery
Hormone pills such as estrogen play a role in ensuring that the uterine lining heals properly after surgery. Medicines can treat pain and other symptoms, too.
Our doctors tailor their approaches to each individual, as the optimal plan often varies widely from one case to the next.
Realistic Treatment Success
Surgical removal of scar tissue returns the majority of patients to normal menstruation. Success rates for restoring fertility are excellent, but no patient will achieve pregnancy.
Determining factors such as age, the extent of scarring, and other health issues are important. While real-world studies continue to find more effective answers, today’s findings emphasize the need for frank discussions about expectations.
Healing Your Uterus Post-Surgery
A successful recovery from surgical treatment of Asherman’s Syndrome requires an intentional approach. Restoring the uterus will be a time-consuming process and usually requires multiple modalities. It’s not a fast process for most—so patience and diligent attention to detail are key.
Because everyone’s journey varies, providers will customize a course of action based on the individual patient—not cookie-cutter. A combination of eastern and western therapies have been useful in my healing journey.
Physical therapy or pelvic floor therapy can help reduce pain and promote healing. In most cases, a small balloon filled with saline is inserted within the uterus for several days after surgery. This prevents the uterine walls from re-attaching, allowing them plenty of space to heal and reducing the chance of creating new adhesions.
Collaboration among OB-GYNs, fertility experts, and therapists is essential to heal the body and mind, providing holistic care that’s vital to overall well-being. Keeping up with follow-up appointments with your physician is important to monitor for new adhesions and the healing of your uterus.
Close monitoring is crucial as a few individuals will require multiple procedures to achieve the desired results.
Supportive Healing Therapies
- Pelvic floor therapy
- Acupuncture
- Yoga and gentle stretching
- Counseling
Complementary therapies such as acupuncture can reduce pain and stress. Many people find that holistic care—particularly mind-body approaches—makes them feel empowered and in control.
New Treatment Frontiers
Doctors are beginning to explore the use of platelet-rich plasma (PRP) and stem cell treatments. While these are not the norm just yet, preliminary research suggests they could improve healing significantly.
High-dose estrogen therapy is another treatment that has been attempted with conflicting success. By keeping an eye on the research, patients can be first in line to explore these new options as they become available.
Lifestyle for Uterine Health
- Eat a balanced diet
- Stay active with gentle exercise
- Avoid tobacco and limit alcohol
- Manage stress
Proper nutrition and movement are crucial to healing the body. Eliminating tobacco and other reproductive toxicants is critical to uterine health and fertility.
Fertility Journey After Asherman’s
It takes time and effort and patience to recover from Asherman’s Syndrome. As a result, most women only experience light or absent menstrual bleeding, making it challenging to monitor progress. As much as we love for it, treatment — such as hysteroscopic adhesiolysis — is only the first step.
Getting back to a normal life isn’t quick or easy, and it requires support from physicians who truly understand this condition.
Tracking Uterine Recovery
After extensive treatment, the uterus will require time to recover. Doctors usually monitor the uterine lining and menstrual flow as indicators that recovery is proceeding normally. This has resulted in some women regaining normal menstrual cycles and others having persistently light or absent periods.
Track Uterine Healing Recovery is different for each person. Many others are looking forward to attempting pregnancy again in a few months. For others, the wait will be longer, particularly if recovery is taking its time or if adhesions reoccur.
Regular follow-up examinations allow issues to be detected early and inform safe next steps.
Timing Conception Attempts
Developing a fertility journey Getting pregnant after Asherman’s takes a lot of planning. Assisted reproductive technologies, such as IVF, become a viable option when natural conception proves difficult or when the uterus is eternally marked by scarring.
A doctor will recommend ART if menstrual cycles do not resume or if multiple miscarriages have occurred. Often, ART is most effective when performed after surgery. Combining the two provides the best chance at achieving a pregnancy.
Every situation is unique.
When ART Can Help
There’s no single correct path to parenthood following Asherman’s. Whether you’re a couple that seeks ART, a couple that achieves naturally, or a couple that does both, ART has an impact.
Emotional support and counseling is extremely important, as the journey can be both lengthy and taxing. Plans will likely pivot, and that’s perfectly fine. Being candid with doctors will address what route will be most effective for you.
Long-Term Fertility Paths
The emotional burden of Asherman’s can be immense. Therapy, open communication with both romantic partners and medical professionals, and medication have all been instrumental.
Given the additional risks associated with these pregnancies, work in tandem with high-risk specialists.
My Take: Navigating Asherman’s
Managing Asherman’s Syndrome means navigating the medical field. It’s a long road indeed, with different hurdles for each individual. The journey to diagnosis and treatment is exhausting. You wait for them, stressing about symptoms such as missed periods or difficulty conceiving, and you wrestle with the anxiety surrounding a rare condition.
Since Asherman’s diagnosis is not straightforward, hysteroscopy serves as the gold standard for diagnosis. Even with treatment, some people need additional procedures as scar tissue is known to reappear. The emotional toll is very real and should not be discounted.
The Unseen Emotional Impact
The emotional toll of infertility is difficult to describe, but heavy is an understatement. It is natural to feel anxiety, sadness, and sometimes guilt during the process of awaiting results or dealing with failures. Countless others have found relief by seeking help from mental health professionals or support groups.
Creating a support network goes a long way. Looking back, I felt completely alone and my hands were tied. She says self-care isn’t one set thing. You may decide to start practicing lighter forms of exercise, meditate and find creative hobbies that keep your mind occupied in a different way.
Emotional support is equally important to physical care.
Choosing Your Medical Team
Getting started with Asherman’s treatment requires the right doctors. Find specialists who have seen the wave highs and lows. Equally, they need to be responsive to your concerns. OB-GYNs paired with fertility experts and mental health professionals, like therapists, psychiatrists, or supportive counselors, create an impactful trifecta.
Open communication is key. Your medical team should walk you through the options in an understandable way. Then they’ll tell you the pros and cons and collaborate to decide the best way to proceed. New therapies—like new money to promote advanced surgical techniques and new products to encourage healing—are more of a conversation.
Be Your Own Advocate
Don’t be afraid to ask questions and seek second opinions. The further along you are with understanding the treatments, the more empowered you’ll feel. You’re going to select options that are just right for you!
So avoiding a late diagnosis and working in partnership with your doctors is essential to achieving a positive outcome and regaining your fertility. Support, education, and being proactive can help turn the tide.
Frequently Asked Questions
What causes Asherman’s syndrome?
What causes Asherman’s syndrome Asherman’s syndrome typically occurs after any type of surgery inside the uterus, especially after a D&C (dilation and curettage). This scarring within the uterus can cause problematic symptoms and issues with fertility.
How is Asherman’s syndrome diagnosed in the U.S.?
Doctors perform hysteroscopy—an office-based procedure—to directly visualize the inside of the uterus. To get a definitive diagnosis, they might order a pelvic ultrasound or an HSG (hysterosalpingogram).
Can Asherman’s syndrome be treated?
Yes. In most cases, the treatment of choice is hysteroscopic surgery to carefully remove scar tissue and restore the uterine cavity. The earlier treatment is done, the better the fertility outcome.
Will treating Asherman’s syndrome restore fertility?
Forty-three percent of women presented with infertility improved fertility post-treatment. For fertility reasons, the sooner it’s removed, the better the chances are for a successful pregnancy.
How long is recovery after Asherman’s surgery?
How long is recovery after Asherman’s surgery? Recovery is typically fast—most women are back to regular activity within a few days. To help your uterus heal, your doctor might put you on estrogen.
Is Asherman’s syndrome common in the United States?
It is uncommon but occurs more frequently following multiple uterine surgeries. If you’ve had several D&Cs, discuss your personal risk with your physician.
Can Asherman’s syndrome come back after treatment?
There’s only a slight risk of scar tissue re-forming. Early detection and treatment is key, which is why routine follow-ups with your fertility specialist after treatment is essential.